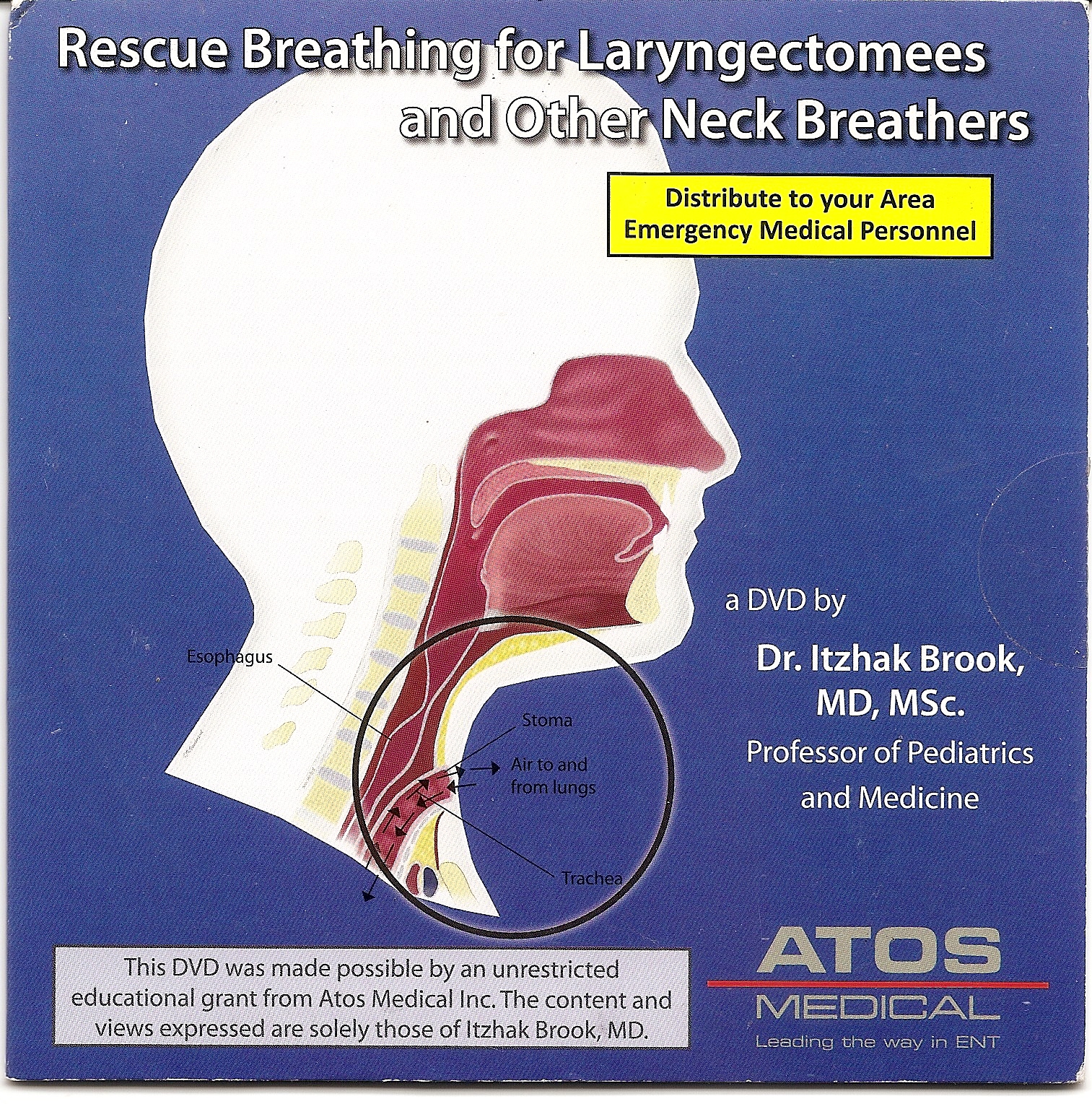
Rescue breathing for laryngectomees and other neck breathers
Laryngectomees and other neck breathers are at great risk of receiving inadequate acute care when they experience breathing difficulties or when they need cardiopulmonary resuscitation (CPR). Emergency departments (EDs) and emergency medical response services (EMS) personnel often do not recognize a patient who is a neck breather, do not know how to administer oxygen in the proper way, and may erroneously give mouth-to-mouth ventilation when mouth-to-stoma ventilation is indicated. This can lead to devastating consequences, depriving sick people from the oxygen needed to survive.
Many medical personnel are not familiar with the care of laryngectomees because a laryngectomy is a relatively rare procedure. Currently laryngeal cancers are detected and treated early. A total laryngectomy is generally indicated only for large tumors or for tumors that recur after previous treatment. There are currently only about 60 000 individuals who have undergone this procedure in the United States. As a result, acute care health providers have less contact than ever with laryngectomees.
This section outlines the special needs of laryngectomees and other neck breathers, explains the anatomical changes after laryngectomy, describes how laryngectomees speak and how to recognize them, outlines how to distinguish between total and partial neck breathers, and describes the procedures and equipment used in rescue breathing for total and partial neck breathers.
Causes of sudden respiratory distress in laryngectomees
The most common indication for a laryngectomy is cancer of the head and neck. Many laryngectomees also suffer from other medical problems resulting from their malignancy and its treatment which often includes radiation, surgery and chemotherapy. Laryngectomees also have difficulties in speaking and must therefore use various methods to communicate.
The most common cause of sudden breathing difficulty in laryngectomees is airway blockage due to aspiration foreign body or a mucus plug. Laryngectomees may also suffer from other medical conditions including heart, lung and vascular problems.
The anatomy after total laryngectomy
The anatomy of laryngectomees is different from the anatomy of those who have not undergone this procedure. After a total laryngectomy, the patient breathes through a stoma (an opening in the neck for the trachea). There is no longer a connection between the trachea and the mouth and nose. Laryngectomees may be difficult to recognize because many cover their stomas with foam covers, ascots, or other garments. Many also apply a Heat and Moisture Exchanger (HME) or a Hands Free device over their stoma.
Anatomy before and after laryngectomy (with the permission of Karen Vanderpool Haerle and Atos Medical)
Differentiation between partial neck breathers and total neck breathers
It is important for medical personnel to differentiate partial neck breathers from total neck breathers (including laryngectomees) because the management of each group is different. The trachea is not connected to the upper airways in total neck breathers and all breathing is done through the tracheostomy site. In contrast, among partial neck breathers, although a tracheostomy site is present, there is still a connection between the trachea and the upper airway. Although partial neck breathers breathe mainly through their stoma, they are also able to breathe through their mouth and nose. The extent of breathing through the upper airways in these individuals varies.
Many partial neck breathers breathe through a tracheostomy tube, which may be protruding from the stoma and is often strapped to the neck. Failure to recognize a partial neck breather may lead to inappropriate treatment.
Anatomy of partial neck breather (with the permission of Atos Medical)
Preparation for rescue breathing
The steps to rescue a neck breather are:
1. Determine the patient's unresponsiveness
2. Activate the emergency medical services
3. Position the person by raising their shoulders
4. Expose the neck and remove anything covering the stoma such as filter or cloth that may prevent access to the airway
5. Secure the airway in the stoma and remove anything blocking the airway such as the filter or HME
6. Clear any mucus from the stoma.
It is not necessary to remove the stoma’s housing unless it blocks the airway. Laryngectomy tubes or stoma buttons may be carefully removed. The voice prosthesis should not be removed, unless it is blocking the airway, since it generally does not interfere with breathing or suctioning. If the prosthesis is dislodged it should be removed and replaced with a catheter to prevent aspiration and fistula closure. If present, the tracheal tube may need to be suctioned after insertion of 2-5 cc of sterile saline or be entirely removed (both outer and inner parts) to clear any mucus plugs. The stoma should be wiped and suctioned. The next step is to listen for breathing sounds over the stoma. If the tracheostomy tube is blocked the chest may fail to rise.
If a tracheostomy tube is used for resuscitation it should be shorter than the regular one so that it can fit the length of the trachea. Care should be used in inserting the tube so that it does not dislodge the voice prosthesis. This may require the use of a tube with a smaller diameter.
If the patient is breathing normally he/she should be treated like any unconscious patient. If prolonged administration of oxygen is require, it should be humidified.
It may be difficult to detect a carotid artery pulse in the neck of some laryngectomees because of post radiation fibrosis. Some patients may not have a radial artery pulse in one of their arms if tissue from that arm was used for a free flap to reconstruct the upper airway.
Ventilation of total neck breathers
CPR for neck breathers is generally similar to CPR performed on normal individuals with one major exception. Neck
breathers are administered ventilation and oxygen through their stoma. This can
be done by a mouth-to-stoma ventilation or by using an oxygen mask
(infant/toddler mask or an adult mask turned 900). It is useless
to try to perform mouth-to-mouth ventilation.
Ventilation of total neck breathers (with the permission of Atos Medical)
Oxygen mask
Infant bag valve mask used in rescue breathing
Ventilation of partial neck breathers
Although partial neck breathers inhale and exhale mainly through their stomas, they still have a connection between their lungs and their noses and mouths. Therefore, air can escape from their mouths and/or noses, thus reducing the efficacy of ventilation. Even though partial neck breathers should receive ventilation through their stomas, their mouths should be kept closed and their noses sealed to prevent air from escaping. This can be done by holding the patient’s mouth and nose tightly closed.
Communication during respiratory distress and medical emergency
Laryngectomees may have difficulties in communication during respiratory distress and medical emergency and if possible they should be allowed to do so by writing or through flash cards. Laryngectomees and other neck breathers can assist in preventing life threatening mishaps by carrying an emergency card, displaying an emergency card in their car, and/or wearing a bracelet or a neck chain that identifies them as a neck breather. It is also important for them to carry a list of their medical conditions, the medication they take, the names of their doctors and contact information. Laryngectomees should also communicate their unique needs ahead of time by calling the 911 services, the police department and the EMS in their community. They or their doctors should contact the EDs in their areas so that their personnel would be able to recognize neck breathers and deliver proper assistance to them.
Emergency department
and EMS personnel should be vigilant in recognizing those who do not breathe through the mouth and nose. The knowledge of health care providers in communities may vary. Many health care providers are not familiar with
the care of neck breathers, although this is taught at CPR courses. Proper administration of oxygen and ventilation through the stoma and specific details of CPR to neck breathers should be practiced periodically. The medical and EMS community should maintain their knowledge about the proper treatment of neck breathers so that effective care of these individuals is provided in urgent circumstances.
Using an emergency alert device can be lifesaving and can alert emergency services about any respiratory and/or medical emergency. Because laryngectomees may have difficulties in communicating
their distress over the phone or give their accurate location, it is preferred to
have an emergency alert device with GPS tracer.
Medical alert device
Alerting others that one needs assistance
can also be done by placing a whistle that is connected to a nipple over the
stoma and forcefully exhaling. (see picture below) It is also possible to blow a
whistle by puffing out the cheeks like blow one blows out a candle while
pinching the nose.
A video presentation of rescue breathing can be watched on YouTube and also obtained by contacting Dr I Brook at
ib6@georgetown.edu
Summary
Laryngectomees and other neck breathers are at great risk of receiving inadequate acute care when they experience breathing difficulties or need cardiopulmonary resuscitation. It is essential that medical personnel learn to identify neck breathers and differentiate partial neck breathers from total neck breathers. Respiratory problems unique to neck breathers include mucus plugs and foreign body aspiration. Although partial neck breathers inhale and exhale mainly through their stomas they still have a connection between their lungs, their noses, and their mouths. In contrast, there is no such connection in total neck breathers. Both partial and total neck breathers should be ventilated through their tracheostomy sites. However, the mouth needs to be closed and the nose sealed in partial neck breathers to prevent escape of air. An infant or toddler bag valve mask should be used in ventilating through the stoma.
Ensuring adequate urgent care for neck breathers including laryngectomees
Neck breathers are at a high risk of receiving inadequate therapy when seeking urgent medical care because of shortness of breath.
It
is common that medical personal mistakenly administered oxygen to
the neck breather through their nose and not through their tracheotomy site.
Neck breathers can
prevent a mishap by:
1. Wearing a bracelet that identifies them as neck breathers.
When hospitalized - w
earing the hospital patient ID wristband on the same hand
that identifies them as neck breathers.
2. Carrying a card with a list describing their medical conditions, their medication, the names of their doctors and their contact information.
3.
Have one’s medical
information and contacts in a health application on their android or IPhone.
4. Placing a sticker on the inside of their car windows identifying them as neck breathers. The card contains information about caring for them in an emergency.
5. Using an
electrolarynx can be helpful and allow communication even in an emergency. Those who use a TEP for speech may not be able to speak because their HME may need to be removed.
6. Placing a note on their front door identifying themselves as a neck breather.
7. Informing the local 911 emergency services, EMSs and police
department that they are neck breathers and may not be able to speak during an emergency. Some 911 centers allow sending text messages instead of calling.
8. Registering with Smart 911 service whenever it is available and providing one's medical
information including that one is a neck breather and may not be able to speak.
9.
Ensuring that the medical personnel
of their local emergency
rooms can recognize and treat neck breathers.
10. When staying in a hotel informing the front desk or the operator that you may not be able to talk in an emergency.
It is up to laryngectomees to be vigilant and increase the awareness of the medical personnel and EMSs in their area. This can be an ongoing task, since knowledge by health providers may vary and change over time.
A
slide presentation, a
video presentation, and an
instructive manual that explain how to recognize, provide respiratory resuscitation, provide oxygen, ventilate and perform CPR to laryngectommes is available in this blog. The slide presentation can be downloaded and saved.
A video that explains the methods needed to administer urgent respiratory care to neck breathers can be
viewed on YouTube.
To obtain a free DVD of the video e mailing a request to
customersupport.us@atosmedical.com
Neck breathers should share these presentations with their emergency care givers (Closest ED and EMS).
Ensuring adequate care during
hospitalization for neck breathers including laryngectomees
Neck breathers are at a high risk of
receiving inadequate care when hospitalized. The medical staff is often not aware
of their condition; do not know how to care of their airways, and how to
communicate with them. It is therefore important to take these steps to ensure
that the care is adequate:
- Informing the ward’s head nurse and attending
physician about the laryngectomee’s general and specific needs. In case of elective admission, this can be
done prior to the admission to allow the staff time to get ready and get
adequate supplies and equipment.
- Informing the dietitian about the food
requirements of the laryngectomee.
- Informing and when possible meet with the
hospital’s speech and language pathologist to insure adequate care and availability
of adequate supplies.
- Laryngectomees who experience swallowing difficulties
should request that the orally administered medications be given in liquid or
easy to swallow form.
- Requesting specific supplies and equipment to
ensure adequate, respiratory care such as saline bullets, humidifier, and
suction machine.
- Keeping reminding every staff member caring for
the laryngctomee about his or her condition. This can be done by the patient
and/or their advocate. Remind the ward’s head nurse, attending physician, and anesthetist (when undergoing a procedure with sedation or surgery) about the proper way of administrating anesthesia, suctioning, ventilating and intubation). Show them the video in YouTube: https://goo.gl/Unstch
- Informing the head nurse, attending physician,
and/or patient’s hospital advocate if medical care is not adequate or errors
are made.
- Requesting that signs informing the staff about
the laryngectomee are placed in the patient’s room. (see pictures below)
- Wearing the hospital patient ID wristband on
the same hand that identifies them as neck breathers. Because staff is required
to continuously check the patient ID wristband, they will be reminded of their
condition. (See picture below)
- Wear a band or bandanna on the forehead that
identifies one as neck breather. (See picture below)
- Making sure that the laryngectomee is able to
communicate with staff. Those using tracheoesophageal speech may need to use
alternative speech methods such as an electrolarynx and/or communicate through writing
and speech generating devices ( i.e., laptop, smartphone, etc.)
- Preparing and bringing adequate supplies required
for their care ( i.e, voice prosthesis and electrolarynx supplies). See section
Preparing a kit with essential information and material when going to the hospital
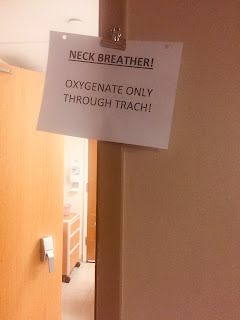

Signs in patient’s hospital room informing the
staff about the laryngectomee
Wearing the hospital patient ID wristband on the
same hand
Wearing band or bandanna on the forehead
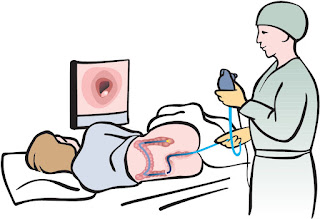
Undergoing a procedure or surgery as a laryngectomee
Undergoing a procedure, (e.g., colonoscopy) by sedation or surgery by either local or general anesthesia
is challenging for laryngectomees.
Unfortunately, most medical personnel who care for laryngectomees before, during, and after
surgery are not familiar with their unique anatomy, how they speak, and how to
manage their airway during and after the procedure or operation. These include nurses,
medical technicians, surgeons and even anesthetists.
It is therefore advisable
that laryngectomees explain their unique needs and anatomy beforehand the
surgery to those who will be treating them. Using explanatory illustrations
or pictures is helpful. Those with voice prostheses should allow their
anesthetist to view their stoma in order to understand its function and be
warned not to remove it. It is helpful to provide the anesthetist the video
that illustrates how to ventilate neck breather ( sending a request to customersupport.us@atosmedical.com ),
or provide them with the link
to it on YouTube.
Medical personnel
should understand that an individual with a total laryngectomy has no connection
between the oropharynx and the trachea and therefore ventilation, administration of oxygen, and airway suctioning should be done through the stoma and not through the nose or mouth.
Undergoing a
procedure with sedation or surgery under local anesthesia is challenging for a laryngectomee because speaking with an electrolarynx or voice prosthesis is generally not
possible. This is because the stoma is covered by an oxygen mask and the patient's hands are typically bound.
However, individuals who use esophageal speech can communicate throughout the
procedure or surgery done under local anesthesia.
It
is important to discuss one’s special requirements with the medical team prior
to surgery. This may require repeating it several times, first to surgeons, than to
the anesthetist in the pre surgical evaluation, and lastly on the day of
surgery to the anesthesia team that is actually going to be in the operating
room. If possible, one could coordinate with the
anesthetist prior to the surgery how to notify him/her of pain, or the need to be suctioned. Hand
signals, head nodding, lip reading or sounds produced by rudimentary esophageal
speech can be helpful.
Using these suggestions may help laryngectomees get adequate care whenever they undergo a medical procedures or surgery done under local anesthesia.

Cardio-Pulmonary Resuscitation (CPR) new guidelines
The American
Heart association (AHA) CPR 2017
guidelines encourages lay people to use cardiac compressions first. The impetus for the recommendation was that it
is better to use the chest compressions method only rather than do nothing. Mouth-to-mouth
breathing is still recommended in the 2022 guidelines. https://www.cprblspros.com/cpr-cheat-sheet-2022
require CPR may also need respiratory ventilation. One of the
common causes of breathing problems in laryngectomees is an airway obstruction
due to a mucus plug or foreign body. Removing these may be essential. Mouth to
stoma resuscitation is important and relatively easier to deliver than mouth
to mouth breathing.
Laryngectomees who breathe through a Heat and
Moisture Exchanger (HME) and perform CPR on a person in need of resuscitation may
need to temporarily take their HME off. This allows laryngectomees to inhale more air when they deliver up to one hundred heart compressions per minute.
Helping a person in distress as a laryngectomee
As a physician I had responded to emergencies on numerous occasions. These were aboard airplanes, and at the side of the road after car accidents. I felt that it was my duty to help others and save lives if needed. After I became a laryngectomee I realized that my ability to help would be curtailed because I would no longer be able to provide mouth to mouth resuscitation if needed. This is why I hesitated for a couple of seconds before I rushed to help a woman who was choking.
This happened at a place where I would have not expected - in the middle of a theater play. It occurred on November 21, 2011 while I was watching a play in theater J in Washington DC. In the second half of the play I heard sounds of commotion in the back of the theater. Suddenly someone yelled: “We need help! Is there a doctor?” The actors stopped the play and one of them repeated the requested for help. I looked at the direction of the commotion and saw a woman who was choking and struggling to breath. I hesitated for a second because I worried that I could not do adequate cardio respiratory resuscitation which included mouth to mouth ventilation. However, knowing that the new American Heart association guidelines require only chest compressions was reassuring because I knew that I could deliver this treatment if needed. I also worried about my ability to communicate with the person in distress. Fortunately, I was speaking through a hands free heat and moisture exchanger (HME) placed on my stoma which allowed me to use both of my hands while speaking, and I was using a waistband voice amplifier which allowed me to be heard in the crowded theater.
No one else in the audience of almost 300 people responded to the call for help. I knew right away I had to act. I quickly climbed the steps toward the woman in need and helped her regain her breathing. Fortunately the problem was not serious and it took only a couple of minutes before she recovered and we were all able to watch the end of the play.
I felt a sense of gratification after the incident not only because I was able to help a person in need but also because I realized that I can still do it as a laryngectomee. This was a healing experience for me as I finally regained my self confidence to respond to emergencies as I did before.



.jpg)
.jpg)



















No comments:
Post a Comment