Risk factors of head and
neck cancers
Alcohol and tobacco use. The two major risk factors for
developing head and neck cancers (HNC) are alcohol and tobacco use. This is
especially true for cancers of the oral cavity, oropharynx, hypopharynx, and
larynx (not salivary gland cancers). It is estimated that at least 75% of head
and neck cancers are caused by tobacco and alcohol use. Using both tobacco and
alcohol places people at higher risk for developing these cancers.
·
Opium
snuffing. Opium dependency increases the
likelihood of developing laryngeal cancer at a younger age.
Human papillomavirus (HPV) is a risk factor for some HNC,
especially oropharyngeal involving the tonsils or the base of the
tongue.
Epstein-Barr virus infection. Infection with the Epstein-Barr virus is a risk factor for nasopharyngeal and salivary glands cancers especially in Chinese and Malays.
Gastroesophageal reflux disease or GERD is a risk factor
for laryngopharyngeal cancer.
Epstein-Barr virus infection. Infection with the Epstein-Barr virus is a risk factor for nasopharyngeal and salivary glands cancers especially in Chinese and Malays.
Radiation exposure. Radiation to the head and neck, for
noncancerous conditions or cancer, is a risk factor for salivary glands cancer.
Oral health. Poor oral hygiene, missing teeth, and using
mouthwash with a high alcohol content are risk factors for oral cavity cancer.
Preserved or salted foods. Consumption of certain preserved or
salted foods during childhood is a risk factor for nasopharyngeal cancer.
Paan (betel quid). Sometimes used in Southeast Asia is
strongly associated with an increased risk of oral cancer.
Occupational exposure. Wood dust is a risk factor for
nasopharyngeal cancer. Asbestos, synthetic fibers, metal, textile, ceramic, and
logging have been associated with cancer of the larynx. Wood, nickel dust, and formaldehyde may increase risk for cancer of the paranasal sinuses and nasal
cavity.
Ancestry. Asian ancestry, particularly Chinese,
is a risk factor for nasopharyngeal cancer.
Maté. A tea-like beverage consumed by South Americans has been
associated with an increased risk of cancers of the mouth, throat, esophagus,
and larynx.

Signs
and symptoms of head and neck cancers
Signs and Symptoms of all head
and neck cancers may include:
- A sore throat that does not go away
- A change or hoarseness in the voice
- A lump or a sore that does not heal
- Difficulty swallowing
- Unintentional weight loss
Sign
and symptoms of specific head and neck cancers:
Laryngeal cancer:
- Pain when swallowing or ear pain
- Difficulty breathing
- Coughing
Oral cavity
- A white or red patch on the gums, tongue, or lining of the mouth
- A swelling of the jaw that causes dentures to fit poorly or become uncomfortable
- Abnormal bleeding or pain in the mouth
Paranasal sinuses and
nasal cavity cancer
- Sinuses that are blocked and do not clear
- Chronic sinus infections that do not respond to treatment with antibiotics
- Blockage in one nostril
- Pus or discharge from the nose
- Mucus draining from the back of the nose into the throat
- Sinus pain
- Nose bleeds
- Frequent headaches
- swelling or other trouble with the eyes
- Pain in the upper teeth
- Loose upper teeth or changes in how dentures fit
·
Salivary glands cancer
- Swelling under the chin or around the jawbone
- Painless lump(s) in the area of the ear, cheek, jaw, lips, or mouth
- Numbness or weakness of the muscles in the face
- Pain in the face, the chin, or the neck that does not go away
- Fluid draining from the ear
- Trouble swallowing
- Difficulty opening the mouth widely
Pharyngeal cancer
- Sore in the mouth or on the lip that does not heal
- Red or white patch on the gums, tongue, tonsil, or lining of the mouth
- Lump on the lip, mouth, neck, or throat or a feeling of thickening in the cheek
- Persistent sore throat or feeling that something is caught in the throat
- Trouble breathing
- Hoarseness or change in voice
- Numbness of the mouth or tongue
- Difficulty in hearing
- Pain or bleeding in the mouth
- Pain in the neck or the throat that does not go away
- Difficulty chewing, swallowing, or moving the jaws or tongue
- Pain when swallowing
- Frequent headaches, pain, or ringing in the ears
- Ear and/or jaw pain
- Chronic bad breath
- Changes in speech
- Loosening of teeth or toothache
- Dentures that no longer fit
- Unexplained weight loss
- Fatigue
- Loss of appetite

Overview of laryngeal cancer
Laryngeal cancer affects the voice box. Cancers that start in the larynx are called laryngeal
cancers; cancers of the hypopharynx are called hypopharyngeal cancers.The hypopharynx is the part of the throat (pharynx) that lies beside and behind the larynx. These cancers are very close to
each other and the treatment principles of both are similar and may involve laryngectomy. Although the discussion below
addresses laryngeal cancer, it is also generally applicable to hypopharyngeal
cancer.
Laryngeal cancer occurs when malignant cells appear in the larynx. The larynx contains the vocal folds (or cords)
which, by vibrating generate sounds that create audible voice when the
vibrations echo through the throat, mouth, and nose.

Laryngeal cancer
The larynx is divided into three anatomical regions: the glottis ( in the middle of the larynx, includes the vocal cords); the supraglottis ( in the top part and includes the epiglottis, arytenoids and aryepiglottic folds, and false cords); and the subglottis
( in the bottom of the larynx). While cancer can develop in any part of the larynx, most laryngeal cancers
originate in the glottis. Supraglottic cancers are less common, and subglottic tumors
are the least frequent.
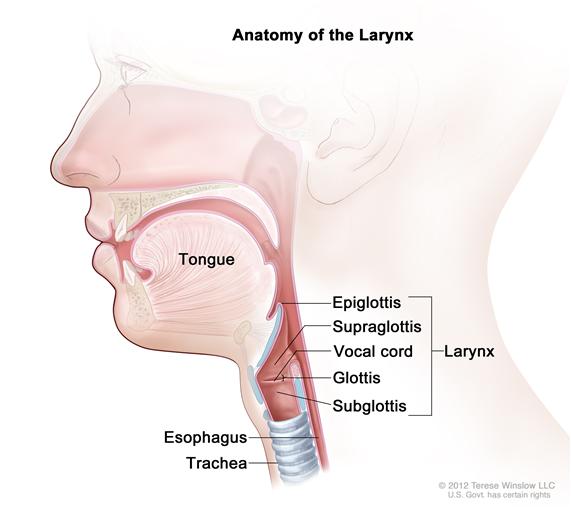
Anatomy of the larynx
Laryngeal and
hypopharyngeal cancer may spread by direct extension to adjacent structures, by metastasis to
regional cervical lymph nodes, or more distantly, through the blood stream to
other locations in the body. Distant metastases to the lungs and liver are most common.
Smoking, and heavy alcohol consumption are the main risk factors
for laryngeal cancer. Exposure to human papilloma virus (HPV) has been mainly associated
with oropharyngeal cancer and to a lesser degree with laryngeal and hypopharyngeal
ones.
There are about 50,000 to 60,000 laryngectomees
in the USA. According to the Surveillance Epidemiology and End Results (SEER) Cancer Statistics Review of the National
Cancer Institute, an estimated 12,250 men and women are diagnosed with cancer
of the larynx each year. In 2023, the rate of new cases of laryngeal
cancer was 2.7 per 100,000 men and women per year, and the death rate was 0.9
per 100,000 men and women per year. Approximately 0.3 percent of men and women
will be diagnosed with laryngeal cancer at some point during their lifetime,
based on 2017–2019 data.The number of new laryngectomees has been declining
mainly because fewer people are smoking and newer therapeutic approaches can
spare the larynx.
Watch video explaining the anatomy of the larynx and symptoms of laryngeal and hypo-pharyngeal
cancer.
Diagnosis
Symptoms and signs of laryngeal cancer include:
Symptoms and signs of laryngeal cancer include:
- Abnormal (high-pitched) breathing sounds
- Chronic cough (with and without blood)
- Difficulty swallowing
- A sensation of a lump in the throat
- Hoarseness that does not get better in 1 - 2 weeks
- Neck and ear pain
- Sore throat that does not get better in 1 - 2 weeks, even with antibiotics
- Swelling or lumps in the neck that does not heal
- Unintentional weight loss
The symptoms associated with laryngeal cancer depend upon its location.
Persistent hoarseness can be the initial complaint in cancers of the glottis. Later
symptoms may include difficulty in swallowing, ear pain, chronic and sometimes bloody
cough, and hoarseness. Supraglottic cancers are frequently diagnosed only when
they cause airway obstruction or palpable metastatic lymph nodes. Primary
subglottic tumors typically present with hoarseness or complaints of difficulty in
breathing on exertion.
There is no single test that can accurately diagnose cancer. The complete evaluation of a patient generally requires a thorough history and physical examination along with diagnostic testing. Many tests are required to determine if a person has cancer or if another condition (such as an infection) may be mimicking the symptoms of cancer.
There is no single test that can accurately diagnose cancer. The complete evaluation of a patient generally requires a thorough history and physical examination along with diagnostic testing. Many tests are required to determine if a person has cancer or if another condition (such as an infection) may be mimicking the symptoms of cancer.
Effective diagnostic testing is used to confirm or eliminate the presence of cancer, monitor its progress, and plan for and evaluate the effectiveness of treatment. In some instances, it is necessary to perform repeat testing if a person’s condition has changed, a sample collected was not of good quality, or an abnormal test result needs to be confirmed. Diagnostic procedures for cancer may include imaging, laboratory tests, tumor biopsy, endoscopic examination, surgery, or genetic testing.
The
following tests and procedures may be used to help diagnose and stage laryngeal
cancer which influences the choice of treatment:
Physical examination of the throat and neck: This enables the doctor to feel for swollen lymph nodes in the neck and to view the throat by using a small, long-handled mirror to check for abnormalities.
Endoscopy: A procedure by which an endoscope (a flexible lighted tube) is inserted through the nose or mouth into the upper airway to the larynx, enabling the examiner to directly view these structures.
Laryngoscopy: A procedure to examine the larynx with a mirror or a laryngoscope (a rigid lighted tube).
CT scan (computed tomography): A procedure that generates a series of detailed radiographs of body sites, taken from different directions. A contrast material such as an injected or swallowed dye enables better visualization of the organs or tissues.
MRI (magnetic resonance imaging): A procedure that uses a magnet and radio waves to generate a series of detailed pictures of areas inside the body.
Barium swallow: A procedure to examine the esophagus and stomach in which the patient drinks a barium solution that coats the esophagus and stomach, and X-rays are obtained.
Biopsy: A procedure where tissues are obtained so that they can be viewed under a microscope to check for cancer.

An upper airway endoscope
The potential for recovery
from laryngeal cancer depends on the following:
- The extent the cancer has spread (the "stage")
- The appearance of the cancer cells (the "grade")
- The location(s) and size of the tumor
- The patient's age, gender, and general health

Microscope used for diagnosing the cancer
Additionally, smoking tobacco and drinking alcohol
decrease the effectiveness of treatment for laryngeal cancer. Patients with
laryngeal cancer who continue to smoke and drink are less likely to be cured
and more likely to develop a second tumor.
Treatment of throat and laryngeal cancers
Individuals with early or small throat or laryngeal cancer may be treated with surgery or radiation therapy. Those with advanced or recurrent cancer may require a combination of treatments. This may include surgery as well as a combination of radiation therapy and chemotherapy generally given at the same time.
Some patients may benefit from second-line therapies that include immunotherapy using checkpoint inhibitors, and anti-epidermal growth factor receptor (EGFR) monoclonal antibodies. Selection of a treatment regimen takes into consideration previous treatment history, patient’s general state and other medical problems, and the potential regimen’s side effects and toxicities.
Checkpoint inhibitors block normal proteins on cancer cells, or the proteins on the T cells that respond to them. These agents strive to overcome one of cancer's main defenses against the individual’s immune system attack. Checkpoint inhibition immunotherapy has been used for the treatment of melanoma, non-small cell lung cancer, renal cell carcinoma, and bladder cancer.
The checkpoint inhibitor Pembrolizumab has been approved for previously treated patients with head and neck squamous cell carcinoma, and clinical trials are ongoing with this and other checkpoint inhibitors. Other trials are currently performed with small molecule tyrosine kinase inhibitors, and anti-EGFR monoclonal antibodies. Patients may chose to enroll in clinical trials of these agents.
Targeted therapy is
another therapeutic option specifically directed at advanced laryngeal cancer. Targeted cancer therapies are administered by using drugs
or other substances that block the growth and spread of cancer by interfering
with specific molecules involved in tumor growth and progression.
The treatment recommendations that are given for a
particular individual's treatment are usually decided at a Tumor Board team
conference where a decision is made usually in accordance with
evidence-based guidelines from the National Comprehensive Cancer Network (NCCN).
Selection of the treatment
regimen takes into consideration the location of the tumor, and whether the
cancer has spread to other sites, previous treatment history, patient’s general
state and other medical problems, and the potential regimen's toxicities.
A team of medical specialists generally collaborate in planning the
treatment.
The team can include:
The team can include:
- Ear, nose, and throat doctor(s) (otolaryngologists)
- General head and neck surgeon(s)
- Medical oncologist(s)
- Radiation oncologist(s)

Other health care providers who work with the
specialists as a team may include a dentist, plastic surgeon, reconstructive
surgeon, speech and language pathologist, physician’s assistant, oncology
nurse, dietitian, certified lymphedema therapist, palliative care, and a social
worker or mental health counselor. Additional team members include primary care
physician, gastroenterologist, pulmonologist, and pain management physician. It is best to have a patient care coordinator that provides coordinated care to the patient by developing, monitoring, and evaluating interdisciplinary care.
Treatment
options depend on the following:
- The extent to which the cancer has spread (the stage)
- The location and size of the tumor
- Whether the cancer has return
- Maintaining the patient's ability to talk, eat, and breathe as normally as possible
- The patient’s general health
- Potential of side effects and toxicity
Other
factors that may be considered include the distance to the treatment center, need for follow-up care, and the availability
of certain procedures at the local facility.
The medical team describes the available treatment choices to the patient and the expected results, as well as the possible side effects. Patients should carefully consider available options and understand how these treatments may affect their ability to eat, swallow, and talk, and whether the treatments will alter their appearance during and after treatment. The patient and his/her health care team can work together to develop a treatment plan that fits the patient's needs and expectations.
The medical team describes the available treatment choices to the patient and the expected results, as well as the possible side effects. Patients should carefully consider available options and understand how these treatments may affect their ability to eat, swallow, and talk, and whether the treatments will alter their appearance during and after treatment. The patient and his/her health care team can work together to develop a treatment plan that fits the patient's needs and expectations.
Supportive care for control of pain and other symptoms that can relieve potential side effects and ease emotional concerns should be
available before, during, and after cancer treatment.
Patients should be well informed before making their choice.
If necessary obtaining a second medical and/or surgical opinion is helpful. Patients are often stressed and
anxious when they learn that they suffer from a serious illness and may not be
able to integrate all the information and explanations they hear. They may therefore
need to hear these several times to integrate the information. Having
a patient advocate (family member or friend) attend the discussions with the medical
team is desirable as they can assist the patient in making the best choice.
It is suggested to ask the following questions of the treatment team:
- What is the size, location,
spread, and stage of the tumor?
- What is the HPV status of the cancer?
- What are the treatment options? Would they include surgery, radiation
therapy, chemotherapy or a combination
of these? Is laryngectomy the only viable option?
- What are the expected side
effects, risks and benefits of each kind of treatment?
- How can side effects be managed?
- What is the risk of recurring cancer?
- What will be the sound of the voice following each of the above treatments?
- What are the chances of being able to eat normally?
- How will the breathing be affected?
- How to prepare for treatment?
- Will the treatment require
hospitalization and if so for how long?
- What is the estimated cost of the
treatment and will insurance cover
it?
- How will the treatment affect one’s
life, work and normal activities?
- Is a research study (clinical
trial) a good option?
- Can the physician recommend an expert for a second
opinion regarding the treatment options?
- How often does the physician and his team take care and/or perform surgery on patients with a similar diagnosis as yours?
- How often and for how long will
there be a need for follow ups?
- Is there a support group in the area that can assist after surgery?

What
to tell your physician
To help one's physicians provide the best care it is helpful to provide them with this information:
- Detailed past medical, dental, social and psychological history
- Detailed description about your symptoms
- Any handicap you have
- Past surgeries
- Past vaccinations
- Medications you take
- Your diet
- Illnesses in your family
- Your work, and travel history (not only recent)
- Exposure to irritants, toxins etc.
- Allergies to food and medications
- Your life style, daily activities, and long term plans
- List of all the physicians and medical care providers
- Your preferred treatment (after hearing the options)
- Your preference knowing details on your condition, treatment and prognosis
- Your preferences about life support
- Your medical insurance coverage
It is a useful to prepare a list of all these issues ahead of time and hand it over to one's physician and other medical providers.

Dealing with psychological and social issues
Learning that one has laryngeal or any head and neck cancer
can change the individual’s life and the lives of those close to them. These
changes can be difficult to deal with. Getting help to better cope with the
psychological and social impact of the diagnosis is very important.
The emotional burden includes concerns about treatment and
its side effects, hospital stays, and the economic impact of the illness
including how to deal with medical bills. Additional worries are directed at how
to care for one’s family, keep one’s work, and continue one's daily
activities.
Sources for support include members of the health care team who can answer and clarify questions about treatment, work, or other activities. Social
workers, counselors, or members of the clergy can be helpful if one wishes to
share his/her feelings or concerns. Social
workers can suggest resources for financial aid, transportation, home care, and
emotional support. Support groups may also offer support in person, over the
telephone, or on the Internet. Member of the health care team can help in finding support groups.

Diagnosis and treatment of recurrent cancer
Recurrent
cancer can occur near the original site of the tumor, known as recurrent local-regional
cancer, or at distant sites in the body, known as recurrent metastatic cancer. Squamous cell carcinomas of the oropharynx associated with human
papillomavirus (HPV) usually have better outcomes that those not associated
with HPV. Patients with these cancers
experience a later onset of distant metastasis and more metastatic sites in
atypical locations.
The symptoms of recurrent cancer can be similar to the primary one or different depending on its location.
Recurrent head and neck cancer is more challenging and difficult than the initial cancer. Treatment options, course and goals depend on whether the recurrence is local, regional or metastatic.
The symptoms of recurrent cancer can be similar to the primary one or different depending on its location.
Recurrent head and neck cancer is more challenging and difficult than the initial cancer. Treatment options, course and goals depend on whether the recurrence is local, regional or metastatic.
The treatment options used for local or regional recurrent head and neck cancer are similar to those used for newly diagnosed disease. These include: surgery, radiation therapy, chemoradiation therapy or chemotherapy, immunotherapy, and targeted agents. However, previously treatment with radiation therapy will influence current treatment choices as it may exclude the patient from additional radiation treatment. However, re-irradiation is possible in some selected cases. Re-irradiation
is more challenging than initial treatment because of the side effects of prior
therapy and concerns about the risks of high cumulative radiation doses to
normal structures.
Unfortunately, the prognosis for recurrent metastatic head and neck cancer is not good. The goals of treatment for recurrent metastatic disease are either to reduce disease symptoms (palliative care), such as pain, and/or to improve survival. Sometime a clinical trial is an optional treatment course. These trials can allow access to new therapies not available to most health care providers or patients, even if it has not yet been determined if the novel therapies will improve outcomes including survival. Decisions about the treatment goals and optimal course of treatment should be made with the patient’s participation.

Additional resources:
Clinical Practice Guidelines for diagnosis, treatment and follow-up. Guidelines of the European Head & Neck Society, European Society for Medical Oncology, and the European Society for Radiology and Oncology.
Machiels JP, René Leemans C, Golusinski W, C Grau C, Licitra L, Gregoire V. Squamous cell carcinoma of the oral
cavity, larynx, oropharynx and hypopharynx: EHNS-ESMO-ESTRO Clinical PracticeGuidelines for diagnosis, treatment and follow-up.
Highlights:
This EHNS-ESMO-ESTRO Clinical Practice
Guideline provides key recommendations for managing SCCHN.
It covers clinical and pathological
diagnosis, staging and risk assessment, treatment and follow-up.
No comments:
Post a Comment