Types of surgery including laryngectomy
Treatment of laryngeal cancer often includes surgery. The surgeon can use either scalpel or laser. Laser microsurgery is performed using a device that generates an intense beam of light that cuts or destroys tissues.
Treatment of laryngeal cancer often includes surgery. The surgeon can use either scalpel or laser. Laser microsurgery is performed using a device that generates an intense beam of light that cuts or destroys tissues.
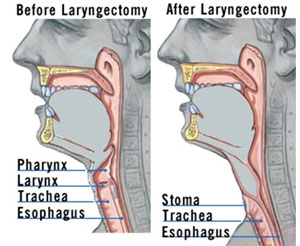
- Removal of the entire larynx (total laryngectomy): The surgeon removes the whole larynx or voice box, along with the entire
pharynx.
- Removal of part of the larynx (open partial laryngectomy): The surgeon takes out only the part of the larynx harboring the tumor.
Total Laryngectomy ( also called laryngectomie, laryngektomie, laringectomia, laryngektomii, Laringektomija, laringektomiya, and larenjektomi) is generally performed for these reasons:
- A large laryngeal untreated cancer that has eroded through cartilage and other structures.
- Laryngeal cancer that came back after previous treatment, (i.e., radiation with/without chemotherapy).
- Prevention of aspiration pneumonia resulting from prior head and neck cancer surgery at sites other the larynx (i.e,. hypopharynx, tongue base).
- Nonfunctional larynx, or inability to eat or drink because of pharyngeal or esophageal strictures.
An incision is made in the central neck,
extending to both sides to perform bilateral neck dissections. The larynx and
neck’s lymph nodes (if needed) and one or both lobes of the thyroid gland are
removed. Frozen sections of the margins of the removed area are studied before
the surgery is complete to determine if no cancer cells are left behind. A laryngostome
is created by sewing the top part of the trachea directly to the skin.
Reconstruction and rehabilitation
procedures might include repair of the pharynx with primary closure, or a flap.
The flap is obtained from other parts of the body and include a pectoralis
major flap, or fee flap recovered from the radial forearm, lateral thigh,
abdominal or scapula area (see below).
A tracheoesophageal puncture might be
done at the same time as the total laryngectomy to assist with speech in the
post-operative time period. A gastric feeding tube is placed either through the
nose, directly in the stomach or inserted through the tracheoesophageal
puncture. Feeding is resumed from a few days to one or two weeks after the
procedure. Small surgical drain(s) are also placed.
Because the parathyroid glands can be
damaged during surgery their activity is monitored by determining calcium serum
levels.
Open Partial Laryngectomy: The main goals of this procedure are to get rid of the cancer
while avoiding a permanent breathing tube in the neck, preserving a suitable
voice and maintaining the ability to swallow. It is limited to small cancers
that have recurred after prior non-surgical therapy. Transoral microsurgery is
another option in these situations.
There are several types of open partial
laryngectomies:
1. Laryngofissure with cordectomy: In this procedure, an incision is made in the midline of the neck,
the thyroid cartilage is split vertically, and the inside of the voice box is exposed
allowing the removal of vocal cord tumors. The thyroid cartilage is then sealed
and the incision is closed. A temporary stent can be placed in in the voice box
for a few weeks to prevent scar band formation. Sometimes a temporary
tracheotomy tube is required.
2. Horizontal laryngectomy: A horizontal partial laryngectomy can be either a supraglottic
hemi-laryngectomy or a supracricoid hemilaryngectomy. This can be performed
with or without resection of the hyoid bone. Following resection, the cricoid
cartilage is sewn back up to the hyoid bone or to the hyoid bone and
epiglottis, depending on what remains after resection of the tumor.
3. Vertical hemi-laryngectomy, or
frontolateral vertical partial laryngectomy: The thyroid
cartilage is exposed following middle neck incision. Then a vertical incision
is made in the thyroid cartilage is incised vertically, and the vocal cord and
arytenoid are removed. Up to 3/4 of the thyroid cartilage can be removed, and
the resection can include a small part of the vocal cord on the other side as
well. Reconstruction can be performed in various ways, including local flaps,
staged procedures and/or free flaps.
4. Transoral laser microsurgery (TLM) with
partial laryngectomy: The procedure is performed through the
mouth using special laryngoscopes, instruments and lasers. It is an option for
small recurrent cancers after non-surgical therapy. In many cases you will
require a tracheotomy, but not all the time. The voice box is exposed using
special instruments. A laser is used to cut out the tumor, with the aim of
getting a margin of normal tissue around it. Associated procedures might
include a tracheotomy, feeding tube placement or a neck dissection - sometimes
performed a few weeks later as a staged neck dissection.
5. Transoral robotic-assisted partial
laryngectomy: This procedure uses a robot to get exposure
and to remove a tumor of the larynx through the mouth. The principles are the
same as transoral laser microsurgery. This procedure is considered experimental
at present. The purpose is to limit incisions and limit dissection of neck
contents.
Lymph nodes that are close or drain the
cancerous site may also be taken out during either type of surgery.
Healing after surgery, and the length of time needed
to recover varies among individuals.
Surgical reconstruction in total laryngectomy
Total laryngectomy is an effective and reliable operation used to remove advanced cancer of the larynx, especially when conservative approaches were unsuccessful. The defect created after the larynx is removed is generally easy to close using sutures or staples. However, when the tumor has spread beyond the larynx and also involves the pharynx or esophagus, such closure is no longer possible and more complex reconstructive options have to be used.
The purpose of reconstruction is to recreate an effective passage through which swallowing as well as esophageal or tracheoesophageal speech are possible. Surgical reconstruction increases surgical time, cost, and postsurgical risks.
When additional tissue is needed to correct the defect, the reconstructive method is affected by the size of the defect, which determines the amount of tissue needed to repair it. The tissue used is called a “flap”. Flaps can be regional (obtained from a site close to the defect) or distal (obtained from a site some distance away from the defect). The blood supply to the flap can either be kept intact (in the regional flap), or the artery and vein serving it need to be connected to the blood supply at the location where it is required. These types of flaps as called “free flaps”.
Pectoralis myocutaneous. This flap has been used for many years and originates from the muscle of the chest and the skin above it. Its advantages are: the excellent and reliable blood supply, availability of sufficient amount of tissue, and proximity to the neck. Its disadvantages include: its large size, the cosmetic deformity it creates by transposing it under the neck skin, and the weakness of the arm it may create.
Deltopectoral flap. Tissues for this flap are taken from deltopectoral muscles region. It is thinner and more closely fits the thin tissue of the pharynx. DP creates minimal donor site problems, but installation of the flap may need to be completed in several stages, and the amount of tissue that can be obtained maybe limited.
Radial forearm free flap. A larger more pliable flap is needed when parts the pharynx or esophagus are removed. This may require using a radial forearm which is obtained from the inside surface of the arm near the wrist. The artery and vein that serve the flap have to be connected to an artery and vein in the neck (a microvascular anastomosis). The donor site is covered with a skin graft taken from another site. This procedure can compromise the blood supply to the hand in individuals with poor hand circulation, and this risk is evaluated prior to considering the RFFF. The first two weeks following surgery are the most vulnerable to blood supply interruption to the flap as the new blood supply may be cut off because of thrombosis. Such interruption has to be addressed promptly to prevent the flap from dying.
Taking one's pulse at the wrist where the flap was obtained is no longer possible after the surgery. It is important to notify one's medical providers about this.
The donor site may feel cold, and since it has no sensation is vulnerable to trauma and frostbite. It should be protected from injury and frostbite by wearing a long shirt and a coat during winter.

The jejunal free flap. The JFF is an alternative to the RFFF. It comes as a cylinder and is especially useful when parts of the esophagus are removed. Although swallowing is generally adequate, the voice is less good as with the RFFF.
In instances where all of the pharynx, larynx, and esophagus are taken out, the stomach can be connected directly to the throat. Because of the potential for a serious infection in the mediastinum after this surgery it is generally used in the most advanced cases where no alternative for reconstruction is available.
The reconstructive options currently available allow for the treatment of more advanced cancer, with a higher likelihood of successful restoration of voicing and swallowing than has been possible in the past. The best option for the patient depends on the tumor’s extent, the risks of each reconstructive option, and the patient’s overall health. Discussion between the patients and surgeon of the risks and benefits of each option can assist in selecting the best one. Obtaining a second option can also assist in the process.

Getting a second opinion
When facing a new medical diagnosis that requires making a choice between several therapeutic options including surgery, it is important to get a second opinion. There may be different medical and surgical approaches and a second (or even third) opinion may be invaluable. Getting such an opinion from physicians experienced in the issues at hand is judicious. There are many situations when treatment cannot be reversed. This is why choosing the course of therapy after consulting with at least one more specialist is very important.
Some individuals may be reluctant to ask for a referral to see another physician for a second opinion. Some may be afraid that this will be interpreted as lack of confidence in their primary physician or doubts about their competence. However, most clinicians welcome and encourage the practice and many medical insurers welcome it.


Surgery's outcome

Side neck view before and after laryngectomy
Surgical reconstruction in total laryngectomy
Total laryngectomy is an effective and reliable operation used to remove advanced cancer of the larynx, especially when conservative approaches were unsuccessful. The defect created after the larynx is removed is generally easy to close using sutures or staples. However, when the tumor has spread beyond the larynx and also involves the pharynx or esophagus, such closure is no longer possible and more complex reconstructive options have to be used.
The purpose of reconstruction is to recreate an effective passage through which swallowing as well as esophageal or tracheoesophageal speech are possible. Surgical reconstruction increases surgical time, cost, and postsurgical risks.
When additional tissue is needed to correct the defect, the reconstructive method is affected by the size of the defect, which determines the amount of tissue needed to repair it. The tissue used is called a “flap”. Flaps can be regional (obtained from a site close to the defect) or distal (obtained from a site some distance away from the defect). The blood supply to the flap can either be kept intact (in the regional flap), or the artery and vein serving it need to be connected to the blood supply at the location where it is required. These types of flaps as called “free flaps”.
The types of available flaps are:
Regional
flaps
· Pectoralis myocutaneous (PMC) flap.
· Deltopectoral (DP) flap.
· Deltopectoral (DP) flap.
Free
flaps
· Radial forearm free flap (RFFF)
· Jejunal free flap (JFF)
Pectoralis myocutaneous. This flap has been used for many years and originates from the muscle of the chest and the skin above it. Its advantages are: the excellent and reliable blood supply, availability of sufficient amount of tissue, and proximity to the neck. Its disadvantages include: its large size, the cosmetic deformity it creates by transposing it under the neck skin, and the weakness of the arm it may create.
Deltopectoral flap. Tissues for this flap are taken from deltopectoral muscles region. It is thinner and more closely fits the thin tissue of the pharynx. DP creates minimal donor site problems, but installation of the flap may need to be completed in several stages, and the amount of tissue that can be obtained maybe limited.
Radial forearm free flap. A larger more pliable flap is needed when parts the pharynx or esophagus are removed. This may require using a radial forearm which is obtained from the inside surface of the arm near the wrist. The artery and vein that serve the flap have to be connected to an artery and vein in the neck (a microvascular anastomosis). The donor site is covered with a skin graft taken from another site. This procedure can compromise the blood supply to the hand in individuals with poor hand circulation, and this risk is evaluated prior to considering the RFFF. The first two weeks following surgery are the most vulnerable to blood supply interruption to the flap as the new blood supply may be cut off because of thrombosis. Such interruption has to be addressed promptly to prevent the flap from dying.
Taking one's pulse at the wrist where the flap was obtained is no longer possible after the surgery. It is important to notify one's medical providers about this.
The donor site may feel cold, and since it has no sensation is vulnerable to trauma and frostbite. It should be protected from injury and frostbite by wearing a long shirt and a coat during winter.

Radial forearm free flap site after surgery (left) and 2 years later
The jejunal free flap. The JFF is an alternative to the RFFF. It comes as a cylinder and is especially useful when parts of the esophagus are removed. Although swallowing is generally adequate, the voice is less good as with the RFFF.
In instances where all of the pharynx, larynx, and esophagus are taken out, the stomach can be connected directly to the throat. Because of the potential for a serious infection in the mediastinum after this surgery it is generally used in the most advanced cases where no alternative for reconstruction is available.
The reconstructive options currently available allow for the treatment of more advanced cancer, with a higher likelihood of successful restoration of voicing and swallowing than has been possible in the past. The best option for the patient depends on the tumor’s extent, the risks of each reconstructive option, and the patient’s overall health. Discussion between the patients and surgeon of the risks and benefits of each option can assist in selecting the best one. Obtaining a second option can also assist in the process.

Preparation of radial forearm free flap site
Preparing for surgery
Prior to surgery it is important to thoroughly discuss with the surgeon all available therapeutic and surgical options and their short and long term outcomes. Patients scheduled for surgery may be anxious and under a lot of stress. It is therefore important to have a patient advocate (such as a family member or friend) also attend the meetings with the surgeon. It is important to freely ask and discuss any concerns and request clarifications. It is necessary to repeatedly listen to explanations until they are understood. It is useful to prepare questions to ask the surgeon and write down the information obtained.
In addition to consultation with the surgeon, it is also important to see these medical providers:
- Internist and/or family physician
- Any specialist one sees for a specific medical problem (i.e., cardiologist, pulmonologis)
- Medical oncologist
- Radiation oncologist
- Anesthetist
- Dentist
- Speech and language pathologist (SLP)
- Social worker or mental health counselor
- Nutritionist
Pre-operative counseling sessions with the patient and family are essential in clarifying what to expect regarding communication restoration. It is also very useful to meet other patients who have already undergone a laryngectomy. These individuals can guide the patient about future speech options, share some of their experiences and provide emotional support.
Contacting a local laryngectomee club to meet other laryngectomees and find support before and after the surgery can be helpful. A list of local laryngectomee clubs in North America and throughout the world is available at the International Association of Laryngectomee website.

The speech and language pathologist (SLP) plays an important role in the care of the total laryngectomy
patients from initiation of pre-operative counseling through acute care, home
health and outpatient services. These includes the pre-laryngectomy evaluation
and education; immediate post-operative care, post-surgical
home care; and post-operative outpatient care. A list of SLP that take care of laryngectomees can be found in the International Association of Laryngectomee website.
Contacting a local laryngectomee club to meet other laryngectomees and find support before and after the surgery can be helpful. A list of local laryngectomee clubs in North America and throughout the world is available at the International Association of Laryngectomee website.

Getting a second opinion
When facing a new medical diagnosis that requires making a choice between several therapeutic options including surgery, it is important to get a second opinion. There may be different medical and surgical approaches and a second (or even third) opinion may be invaluable. Getting such an opinion from physicians experienced in the issues at hand is judicious. There are many situations when treatment cannot be reversed. This is why choosing the course of therapy after consulting with at least one more specialist is very important.
The second doctor may agree with the first doctor’s diagnosis and treatment plan. Conversely, the other physician may suggest a different approach. Either way, the patient ends up with more valuable information and also with a greater sense of control. Eventually one may feel more confident about the decisions he/she makes, knowing that all options have been considered.
Gathering one's medical records and seeing another physician may take some time and effort. Generally, the delay in initiating treatment will not make the eventual treatment less effective. However, one should discuss any possible delay with the physician.
Gathering one's medical records and seeing another physician may take some time and effort. Generally, the delay in initiating treatment will not make the eventual treatment less effective. However, one should discuss any possible delay with the physician.
There are numerous ways to find an expert for a second opinion. One can request a referral to another specialist from the primary doctor, a local or state medical society, a nearby hospital, or a medical school.
Even though patients with cancer are often in a rush to get treated and remove the cancer as soon as possible - waiting for another opinion may be worthwhile.

Recovery
from surgery
The patient's course of recovery depends on the extent of the surgery and reconstruction. After some
surgeries, it is possible to be discharged after several hours of observation
in the recovery room, while other surgeries may require a hospital stay for 7
to 14 days. A longer stay may be needed because of post-operative complications.
Hospital
recovery takes place in different parts of the medical center. Patients are
first observed in the recovery room, than they are moved to the intensive care
unit, and lastly to the regular surgical or otolaryngological ward. Each move
is made when the time is right. With time the lines, tubes, catheters and
drains are gradually removed, and the patient is eventually helped to get up
and walk.
The
post-surgical complications following laryngectomy include: local bleeding (including
hematoma), wound infection, poor wound healing, salivary fistula, low calcium levels (hypocalcemia),
hypothyroidism, blood clots, and aspiration (after partial laryngectomy).
Patients
are discharge from the hospital once the physician(s) determine that there is
no longer a need for in-patient level care. Some patients can go home directly
from the hospital with or without visiting nurses; others might need to be transferred to a
rehabilitation or skilled nursing facility before going home.
Selection of the best discharge location is made by the medical team that is
made of physicians, social workers, nurses and physical therapists. It is made
in conjunction with the patient and his/her family.
A
speech and language pathologist is also involved to assisting the patient to learn about speaking options. An electrical larynx (electrolarynx) can be
used to speak within a few days after the surgery. Because of neck swelling and
post surgical stitches the intra-oral route of delivering vibrations with a
straw-like tube is preferred.
Further
reconstructive and cosmetic procedures or treatments are generally done after
discharge. This allows the patent time for recovery from the initial surgery, get the
pathological results from specimens obtained during the surgery, and make any arrangements needed for the next
steps.

After surgery
Surgery's outcome
The surgery can result in all or some of the following:
- Throat and neck swelling
- Local pain
- Tiredness
- Increased mucus production
- Changes in physical appearance
- Numbness, muscle stiffness and weakness
- Tracheostomy
Most people feel weak or tired for some time after surgery, have a swollen
neck, and experience pain and discomfort for the first few days. Pain medications
can relieve some of these symptoms.
Surgery can alter the ability to swallow, eat, and talk. However,
not all such effects are permanent, as discussed in the Eating and Swallowing page. outcome of surgery page. Those who lose their ability to talk after
surgery may find it useful to communicate by writing on a notepad, writing
board (such as a magic slate), cell phone, or computer. They can also utilize speech generating devices (see page 96) such as laptop, and smartphone. Prior to the surgery it
may be helpful to make a recording for one's answering machine or voicemail to
inform callers about one's speaking difficulties.
An electrolarynx can be used to speak within a few days
after the surgery. (See methods of speaking section chapter) Because of neck swelling and post
surgical stitches, the intra-oral route of delivering vibrations using a
straw-like tube is preferred.


Long
term survival
The
prognosis of head and neck squamous cell carcinoma depends on the
cancer’s stage at diagnosis and its location. Survival rates represent the
percentage of people who are alive within a certain period of time after
treatment, but they should not be used to predict how cancer will affect a
particular patient. Five-year overall survival in patients with stage I or
stage II cancer is generally 70 - 90%. More advanced (stage III or IV) cancer
and those who continue to smoke and consume alcohol have a poorer prognosis.
Those with advanced laryngeal carcinoma have about 40 % five years survival.
The
prognosis is better in HPV associated oropharyngeal cancers compared to non-
HPV associated oropharyngeal cancers.
A
tool that allows general calculation of the expected survival rates of head and
neck cancer patients is available.
In
general, the frequency of follow-up is greatest in the first two to four years
following diagnosis because about 80 to 90% of all recurrences occur within
this period. However, follow-up beyond five years is warranted because of the
risks of late complications, late recurrence, and second malignancies. This is
especially important for patients with non-HPV associated oropharyngeal
cancers.

Pain management after surgery
The degree of pain experienced after laryngecomy (or any other head and neck surgery) is very subjective, but as a general rule, the more extensive the surgery, the more likely the patient will experience pain. Certain types of reconstructive procedures, where tissue is transferred as a flap from the chest muscles, forearm, thigh, jejunum, or a stomach pull up are more likely to be associated with increased or prolonged pain.
Those who have a radical neck dissection as part of the surgery may experience additional pain. At present, most patients undergo a "modified radical neck dissection" where the spinal accessory nerve is not removed. If the spinal accessory nerve is cut or removed during surgery, the patient is more likely to have shoulder discomfort, stiffness, and long term loss of range of motion. Some of the attendant discomfort of this procedure can be prevented by exercise and physical therapy.
For individuals who experience chronic pain as a result of laryngectomy or any other head and neck surgery, evaluation by a pain management specialist is usually very helpful.

No comments:
Post a Comment